Fallen Arches Causes, Signs And Therapy
Overview
It is rare to find someone who walks with both feet in perfect alignment. Often we walk on the inside or outsides of our feet, or with our toes or heels rotated inward. These typical walking patterns can cause many problems not just with the feet but also for the whole body as the alignment of the feet sets the foundation for the whole body?s alignment. One of the most common effects of improper alignment is known as flatfoot, or fallen arches.
Causes
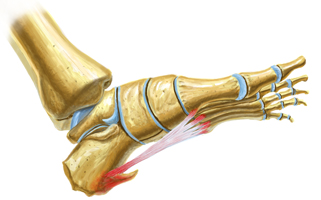
Flat feet in adults can arise from a variety of causes. Here are the most common. An abnormality that is present from birth, stretched or torn tendons, damage or inflammation of the posterior tibial tendon (PTT), which connects from your lower leg, along your ankle, to the middle of the arch, broken or dislocated bones. Some health conditions, such as rheumatoid arthritis, Nerve problems. Other factors that can increase your risk include obesity, diabetes, ageing and Pregnancy.
Symptoms
The primary symptom of fallen arches is painful or achy feet in the area in which the foot arches or on the heel. This area may become swollen and painful to stand still on. This causes the patient to improperly balance on their feet which in turn will cause other biomechanical injuries such as back, leg and knee pain.
Diagnosis
Diagnosis of flat feet or fallen arches can be made by your health practitioner and is based on the following. Clinical assessment involving visual gait assessment, as well as biomechanical assessment. A detailed family and medical history. A pain history assessment determining the location of painful symptoms. Physical palpation of the feet and painful areas. Imaging such as MRI or x-ray can be used by your practitioner to assist in the diagnosis.
fallen arches shoes
Non Surgical Treatment
Treatment for flat feet and fallen arches depends on the severity and cause of the problem. If flat feet cause no pain or other difficulties, then treatment is probably not needed. In other cases, your doctor may suggest one or more of these treatments. Rest and ice to relieve pain and reduce swelling, stretching exercises, pain relief medications, such as nonsteroidal anti-inflammatories, physical therapy, orthotic devices, shoe modifications, braces, or casts, injected medications to reduce inflammation, such as corticosteroids. If pain or foot damage is severe, your doctor may recommend surgery.
Surgical Treatment

In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Prevention
It?s time to take a long hard look at what?s in your closet. Now is the time to toss out shoes that are well worn. You also need to say good-bye to thin-soled shoes that offer zero arch support. If you?re overweight, fallen arches may be a sign the universe is trying to tell you something. You need to lose weight, and odds are, fallen arches are but one of many physical discomforts you are experiencing.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
It is rare to find someone who walks with both feet in perfect alignment. Often we walk on the inside or outsides of our feet, or with our toes or heels rotated inward. These typical walking patterns can cause many problems not just with the feet but also for the whole body as the alignment of the feet sets the foundation for the whole body?s alignment. One of the most common effects of improper alignment is known as flatfoot, or fallen arches.
Causes
Flat feet in adults can arise from a variety of causes. Here are the most common. An abnormality that is present from birth, stretched or torn tendons, damage or inflammation of the posterior tibial tendon (PTT), which connects from your lower leg, along your ankle, to the middle of the arch, broken or dislocated bones. Some health conditions, such as rheumatoid arthritis, Nerve problems. Other factors that can increase your risk include obesity, diabetes, ageing and Pregnancy.
Symptoms
The primary symptom of fallen arches is painful or achy feet in the area in which the foot arches or on the heel. This area may become swollen and painful to stand still on. This causes the patient to improperly balance on their feet which in turn will cause other biomechanical injuries such as back, leg and knee pain.
Diagnosis
Diagnosis of flat feet or fallen arches can be made by your health practitioner and is based on the following. Clinical assessment involving visual gait assessment, as well as biomechanical assessment. A detailed family and medical history. A pain history assessment determining the location of painful symptoms. Physical palpation of the feet and painful areas. Imaging such as MRI or x-ray can be used by your practitioner to assist in the diagnosis.
fallen arches shoes
Non Surgical Treatment
Treatment for flat feet and fallen arches depends on the severity and cause of the problem. If flat feet cause no pain or other difficulties, then treatment is probably not needed. In other cases, your doctor may suggest one or more of these treatments. Rest and ice to relieve pain and reduce swelling, stretching exercises, pain relief medications, such as nonsteroidal anti-inflammatories, physical therapy, orthotic devices, shoe modifications, braces, or casts, injected medications to reduce inflammation, such as corticosteroids. If pain or foot damage is severe, your doctor may recommend surgery.
Surgical Treatment
In cases of flat feet that have progressed substantially or have failed to improve with non-surgical treatment, surgery may be required and in some advanced cases, surgery may be the only option. Your foot and ankle surgeon will determine the best approach for you.
Prevention
It?s time to take a long hard look at what?s in your closet. Now is the time to toss out shoes that are well worn. You also need to say good-bye to thin-soled shoes that offer zero arch support. If you?re overweight, fallen arches may be a sign the universe is trying to tell you something. You need to lose weight, and odds are, fallen arches are but one of many physical discomforts you are experiencing.
After Care
Patients may go home the day of surgery or they may require an overnight hospital stay. The leg will be placed in a splint or cast and should be kept elevated for the first two weeks. At that point, sutures are removed. A new cast or a removable boot is then placed. It is important that patients do not put any weight on the corrected foot for six to eight weeks following the operation. Patients may begin bearing weight at eight weeks and usually progress to full weightbearing by 10 to 12 weeks. For some patients, weightbearing requires additional time. After 12 weeks, patients commonly can transition to wearing a shoe. Inserts and ankle braces are often used. Physical therapy may be recommended. There are complications that relate to surgery in general. These include the risks associated with anesthesia, infection, damage to nerves and blood vessels, and bleeding or blood clots. Complications following flatfoot surgery may include wound breakdown or nonunion (incomplete healing of the bones). These complications often can be prevented with proper wound care and rehabilitation. Occasionally, patients may notice some discomfort due to prominent hardware. Removal of hardware can be done at a later time if this is an issue. The overall complication rates for flatfoot surgery are low.
Do You Understand Heel Pain And Discomfort?
Overview

Heel pain can vary from moderate to severe pain that can make walking and daily tasks a chore if not treated. There are a number of different conditions which can cause heel pain so it is important that your heel is properly assessed and diagnosed by a Podiatrist. The most common cause of heel pain is plantar fasciitis. This is where the tissue becomes inflamed at the heel bone or along sole of the foot between the heel and toe. Another condition commonly referred to as a heel spur can also cause pain in the heel. A heel spur is when a spike of bone has been pulled away from the heel bone, where the plantar fascia inserts, causing pain in the area directly under the heel on direct pressure.
Causes
some heel pain can be caused by rheumatological diseases, and these pains can do a real good impersonation of plantar fasciitis symptoms. Seronegative Arthropathies such as Psoriatic Arthritis, Reactive Arthritis and Ankylosing Spondylisis are the most common types to cause heel pain by producing an inflammatory reaction where the fascia attaches to the heel. This is called an enthesitis. If you have a history of Psoriasis or a family history of other arthritic conditions listed above we recommend you see a clinician about your heel pain to confirm the diagnosis. Another occasional cause of heel pain is loss of the cushioning fat pad of the heel, which can result in a bruised heel bone (calcaneus). If you can easily feel your heel bone through your skin on the bottom of your foot you may well have poor fatty tissue on your heel. Pressing on the centre of your heel should feel like pushing into firm rubber, and your skin should not move easily. If you can pinch the skin under your heel and feel a very hard lump when you press the bottom of your heel then it is likely you have a heel fat pad problem. One simple final test is to walk on a hard floor. If you feel the pain only when your heel hits the ground a fat pad problem is most likely. If the pain mainly occurs as you lift the heel off the ground it is more likely to be plantar fasciitis.
Symptoms
Symptoms may also include swelling that is quite tender to the touch. Standing, walking and constrictive shoe wear typically aggravate symptoms. Many patients with this problem are middle-aged and may be slightly overweight. Another group of patients who suffer from this condition are young, active runners.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
Initial treatment consists of rest, use of heel cushions to elevate the heel (and take tension off the Achilles), stretching and applying ice to the area. You can ice and stretch the area simultaneously by filling a bucket with ice and cold water and placing the foot flexed with the toes upward so that the Achilles tendon region is bathed in the cold water for 10 to 15 minutes twice a day. The Achilles region can also become inflamed around the tendon, called paratendinosis. This condition can be treated with the ice bucket stretching, rest and physical therapy. Another area that is commonly subjected to problems is the attachment of the Achilles near or on the heel bone. The heel (calcaneus) itself can have an irregular shape to it, causing irritation to the Achilles as it twists over the region and inflames the bursa, a naturally occurring cushion. Shoes can often aggravate this condition. Sometimes over-stretching, such as the Achilles stretch with the knee bent, can irritate the tendon and cause a bursitis. Prescription foot orthoses can help reduce the torque of the Achilles tendon in these types of cases. Often, the Achilles tendon calcifies near its attachment due to constant torque and tension. Repetitive stress can cause this calcific spur to crack, creating a chronic inflammatory situation that can require surgery. All of these types of chronic Achilles tendinosis that require surgery are successfully treated in over 90 percent of the cases. As with most foot surgery, complete recovery can take up to a year. Though heel pain is common and can be chronic, it does not have to be your weakness (as was the case with the warrior Achilles from Greek mythology).
Surgical Treatment
At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering.
no foot pain
Prevention

The following steps will help prevent plantar fasciitis or help keep the condition from getting worse if you already have it. The primary treatment is rest. Cold packs application to the area for 20 minutes several times a day or after activities give some relief. Over-the-counter pain medications can help manage the pain, consult your healthcare professional. Shoes should be well cushioned, especially in the midsole area, and should have the appropriate arch support. Some will benefit from an orthotic shoe insert, such as a rubber heel pad for cushioning. Orthotics should be used in both shoes, even if only one foot hurts. Going barefoot or wearing slipper puts stress on your feet. Put on supportive shoes as soon as you get out of bed. Calf stretches and stretches using a towel (place the towel under the ball of your feet and pull gently the towel toward you and hold a few seconds) several times a day, especially when first getting up in the morning. Stretching the Achilles tendon at the back of the heel is especially important before sports, but it is helpful for nonathletes as well. Increasing your exercise levels gradually. Staying at a healthy weight. Surgery is very rarely required.
Heel pain can vary from moderate to severe pain that can make walking and daily tasks a chore if not treated. There are a number of different conditions which can cause heel pain so it is important that your heel is properly assessed and diagnosed by a Podiatrist. The most common cause of heel pain is plantar fasciitis. This is where the tissue becomes inflamed at the heel bone or along sole of the foot between the heel and toe. Another condition commonly referred to as a heel spur can also cause pain in the heel. A heel spur is when a spike of bone has been pulled away from the heel bone, where the plantar fascia inserts, causing pain in the area directly under the heel on direct pressure.
Causes
some heel pain can be caused by rheumatological diseases, and these pains can do a real good impersonation of plantar fasciitis symptoms. Seronegative Arthropathies such as Psoriatic Arthritis, Reactive Arthritis and Ankylosing Spondylisis are the most common types to cause heel pain by producing an inflammatory reaction where the fascia attaches to the heel. This is called an enthesitis. If you have a history of Psoriasis or a family history of other arthritic conditions listed above we recommend you see a clinician about your heel pain to confirm the diagnosis. Another occasional cause of heel pain is loss of the cushioning fat pad of the heel, which can result in a bruised heel bone (calcaneus). If you can easily feel your heel bone through your skin on the bottom of your foot you may well have poor fatty tissue on your heel. Pressing on the centre of your heel should feel like pushing into firm rubber, and your skin should not move easily. If you can pinch the skin under your heel and feel a very hard lump when you press the bottom of your heel then it is likely you have a heel fat pad problem. One simple final test is to walk on a hard floor. If you feel the pain only when your heel hits the ground a fat pad problem is most likely. If the pain mainly occurs as you lift the heel off the ground it is more likely to be plantar fasciitis.
Symptoms
Symptoms may also include swelling that is quite tender to the touch. Standing, walking and constrictive shoe wear typically aggravate symptoms. Many patients with this problem are middle-aged and may be slightly overweight. Another group of patients who suffer from this condition are young, active runners.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
Initial treatment consists of rest, use of heel cushions to elevate the heel (and take tension off the Achilles), stretching and applying ice to the area. You can ice and stretch the area simultaneously by filling a bucket with ice and cold water and placing the foot flexed with the toes upward so that the Achilles tendon region is bathed in the cold water for 10 to 15 minutes twice a day. The Achilles region can also become inflamed around the tendon, called paratendinosis. This condition can be treated with the ice bucket stretching, rest and physical therapy. Another area that is commonly subjected to problems is the attachment of the Achilles near or on the heel bone. The heel (calcaneus) itself can have an irregular shape to it, causing irritation to the Achilles as it twists over the region and inflames the bursa, a naturally occurring cushion. Shoes can often aggravate this condition. Sometimes over-stretching, such as the Achilles stretch with the knee bent, can irritate the tendon and cause a bursitis. Prescription foot orthoses can help reduce the torque of the Achilles tendon in these types of cases. Often, the Achilles tendon calcifies near its attachment due to constant torque and tension. Repetitive stress can cause this calcific spur to crack, creating a chronic inflammatory situation that can require surgery. All of these types of chronic Achilles tendinosis that require surgery are successfully treated in over 90 percent of the cases. As with most foot surgery, complete recovery can take up to a year. Though heel pain is common and can be chronic, it does not have to be your weakness (as was the case with the warrior Achilles from Greek mythology).
Surgical Treatment
At most 95% of heel pain can be treated without surgery. A very low percentage of people really need to have surgery on the heel. It is a biomechanical problem and it?s very imperative that you not only get evaluated, but receive care immediately. Having heel pain is like having a problem with your eyes; as you would get glasses to correct your eyes, you should look into orthotics to correct your foot. Orthotics are sort of like glasses for the feet. They correct and realign the foot to put them into neutral or normal position to really prevent heel pain, and many other foot issues. Whether it be bunions, hammertoes, neuromas, or even ankle instability, a custom orthotic is something worth considering.
no foot pain
Prevention
The following steps will help prevent plantar fasciitis or help keep the condition from getting worse if you already have it. The primary treatment is rest. Cold packs application to the area for 20 minutes several times a day or after activities give some relief. Over-the-counter pain medications can help manage the pain, consult your healthcare professional. Shoes should be well cushioned, especially in the midsole area, and should have the appropriate arch support. Some will benefit from an orthotic shoe insert, such as a rubber heel pad for cushioning. Orthotics should be used in both shoes, even if only one foot hurts. Going barefoot or wearing slipper puts stress on your feet. Put on supportive shoes as soon as you get out of bed. Calf stretches and stretches using a towel (place the towel under the ball of your feet and pull gently the towel toward you and hold a few seconds) several times a day, especially when first getting up in the morning. Stretching the Achilles tendon at the back of the heel is especially important before sports, but it is helpful for nonathletes as well. Increasing your exercise levels gradually. Staying at a healthy weight. Surgery is very rarely required.
Workout Routines For Leg Length Discrepancy After Having A Broken Femur
Overview
Leg length discrepancy (LLD) affects about 70% of the general population, and can be either structural - when the difference occurs in bone structures - or functional, because of mechanical changes at the lower limbs. The discrepancy can be also classified by its magnitude into mild, intermediate, or severe. Mild LLD has been particularly associated with stress fracture, low back pain and osteoarthritis, and when the discrepancy occurs in subjects whose mechanical loads are increased by their professional, daily or recreational activities, these orthopaedic changes may appear early and severely. The aim of this study was to analyze and compare ground reaction force (GRF) during gait in runners with and without mild LLD. Results showed that subjects with mild LLD of 0.5 to 2.0 cm presented higher values of minimum vertical GRF (0.57 ? 0.07 BW) at the shorter limb compared to the longer limb (0.56 ? 0.08 BW) Therefore, subjects with mild LLD adopt compensatory mechanisms that cause additional overloads to the musculoskeletal system in order to promote a symmetrical gait pattern as showed by the values of absolute symmetric index of vertical and horizontal GRF variables.
Causes
An anatomical short leg is due to several orthopedic or medical condition mechanisms. Often, one leg simply stops growing before the other one does and is called ?congenital?. We often see mother-daughters or father-sons who exhibit virtually the same degree of shortness on the same side. Often it is not known why this occurs, but it seems to account for approximately 25% of the population demonstrating a true LLD. Other causes of a true LLD include trauma or broken bones, surgical repair, joint replacement, radiation exposure, tumors or Legg-Calves-Perthes disease.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, such as orthotics, epiphysiodesis, shortening, and lengthening, which can be used alone or combined in an effort to achieve equalization of leg lengths. Leg length inequality of 2 cm or less is usually not a functional problem. Often, leg length can be equalized with a shoe lift, which usually corrects about two thirds of the leg length inequality. Up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear. Leg length inequalities beyond 5 cm are difficult to treat with a shoe lift. The shoe looks unsightly, and often the patient complains of instability with such a large lift. A foot-in-foot prosthesis can be used for larger leg length inequalities. This is often done as a temporizing measure for young children with significant leg length inequalities. The prosthesis is bulky, and a fixed equinus contracture may result.

how can i increase my height after 18?
Surgical Treatment
The type of surgery depends on the type of problem. Outpatient procedures may be used to alter the growth of the limb. This is often done through small incisions. If an outpatient procedure is done, your child can continue with most regular activities. Other times, surgery may be very involved and require the use of an external device that is attached to the limb with pins and wires. This device may be left on for months to correct the deformity or lengthen the leg. If this type of surgery is required, your child will be making weekly visits to Cincinnati Children's.
Leg length discrepancy (LLD) affects about 70% of the general population, and can be either structural - when the difference occurs in bone structures - or functional, because of mechanical changes at the lower limbs. The discrepancy can be also classified by its magnitude into mild, intermediate, or severe. Mild LLD has been particularly associated with stress fracture, low back pain and osteoarthritis, and when the discrepancy occurs in subjects whose mechanical loads are increased by their professional, daily or recreational activities, these orthopaedic changes may appear early and severely. The aim of this study was to analyze and compare ground reaction force (GRF) during gait in runners with and without mild LLD. Results showed that subjects with mild LLD of 0.5 to 2.0 cm presented higher values of minimum vertical GRF (0.57 ? 0.07 BW) at the shorter limb compared to the longer limb (0.56 ? 0.08 BW) Therefore, subjects with mild LLD adopt compensatory mechanisms that cause additional overloads to the musculoskeletal system in order to promote a symmetrical gait pattern as showed by the values of absolute symmetric index of vertical and horizontal GRF variables.
Causes
An anatomical short leg is due to several orthopedic or medical condition mechanisms. Often, one leg simply stops growing before the other one does and is called ?congenital?. We often see mother-daughters or father-sons who exhibit virtually the same degree of shortness on the same side. Often it is not known why this occurs, but it seems to account for approximately 25% of the population demonstrating a true LLD. Other causes of a true LLD include trauma or broken bones, surgical repair, joint replacement, radiation exposure, tumors or Legg-Calves-Perthes disease.
Symptoms
Faulty feet and ankle structure profoundly affect leg length and pelvic positioning. The most common asymmetrical foot position is the pronated foot. Sensory receptors embedded on the bottom of the foot alert the brain to the slightest weight shift. Since the brain is always trying to maintain pelvic balance, when presented with a long left leg, it attempts to adapt to the altered weight shift by dropping the left medial arch (shortening the long leg) and supinating the right arch to lengthen the short leg.1 Left unchecked, excessive foot pronation will internally rotate the left lower extremity, causing excessive strain to the lateral meniscus and medial collateral knee ligaments. Conversely, excessive supination tends to externally rotate the leg and thigh, creating opposite knee, hip and pelvic distortions.
Diagnosis
The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear.
Non Surgical Treatment
Treatment of leg length inequality involves many different approaches, such as orthotics, epiphysiodesis, shortening, and lengthening, which can be used alone or combined in an effort to achieve equalization of leg lengths. Leg length inequality of 2 cm or less is usually not a functional problem. Often, leg length can be equalized with a shoe lift, which usually corrects about two thirds of the leg length inequality. Up to 1 cm can be inserted in the shoe. For larger leg length inequalities, the shoe must be built up. This needs to be done for every shoe worn, thus limiting the type of shoe that the patient can wear. Leg length inequalities beyond 5 cm are difficult to treat with a shoe lift. The shoe looks unsightly, and often the patient complains of instability with such a large lift. A foot-in-foot prosthesis can be used for larger leg length inequalities. This is often done as a temporizing measure for young children with significant leg length inequalities. The prosthesis is bulky, and a fixed equinus contracture may result.
how can i increase my height after 18?
Surgical Treatment
The type of surgery depends on the type of problem. Outpatient procedures may be used to alter the growth of the limb. This is often done through small incisions. If an outpatient procedure is done, your child can continue with most regular activities. Other times, surgery may be very involved and require the use of an external device that is attached to the limb with pins and wires. This device may be left on for months to correct the deformity or lengthen the leg. If this type of surgery is required, your child will be making weekly visits to Cincinnati Children's.
True Apparent Leg Length Discrepancy
Overview
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
The most common symptom of all forms of LLD is chronic backache. In structural LLD the sufferer may also experience arthritis within the knee and hip are, flank pain, plantar fasciitis and metatarsalgia all on the side that is longer. Functional LLD sufferers will see similar conditions on the shorter side.
Diagnosis
Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue.
Non Surgical Treatment
The object of treatment for leg length discrepancy is to level the pelvis and equalize the length of the two limbs. Inequalities of 2-2.5 centimeters can be handled with the following. Heel lifts/ adjustable heel lifts can be used inside a shoe where shoes have a full heel counter. Heel lifts may be added to the heel on the outside of the shoe along with an internal heel lift. Full platforms along the forefoot and rearfoot area of a shoe can be added. There are many different adjustable heel lifts available on the market. For treatment of a leg length discrepancy, consult your physician. They may refer you to a Physiotherapist or Chiropractor for determination of the type of LLD. A Certified Pedorthist (Canada) will treat a structural leg length discrepancy with a heel lift or in larger discrepancies a footwear modification.
how can a woman look taller?
Surgical Treatment
Surgeries for LLD are designed to do one of three general things ? shorten the long leg, stop or slow the growth of the longer or more rapidly growing leg, or lengthen the short leg. Stopping the growth of the longer leg is the most commonly utilized of the three approaches and involves an operation known as an epiphysiodesis , in which the growth plate of either the lower femur or upper tibia is visualized in the operating room using fluoroscopy (a type of real-time radiographic imaging) and ablated , which involves drilling into the region several times, such that the tissue is no longer capable of bone growth. Because the epiphyseal growth capabilities cannot be restored following the surgery, proper timing is crucial. Usually the operation is planned for the last 2 to 3 years of growth and has excellent results, with children leaving the hospital within a few days with good mobility. However, it is only appropriate for LLD of under 5cm.
Shortening techniques can be used after skeletal maturity to achieve leg length equality. Shortening can be done in the proximal femur using a blade plate or hip screw, in the mid-diaphysis of the femur using a closed intramedullary (IM) technique, or in the tibia. Shortening is an accurate technique and involves a much shorter convalescence than lengthening techniques. Quadriceps weakness may occur with femoral shortenings, especially if a mid-diaphyseal shortening of greater than 10% is done. If the femoral shortening is done proximally, no significant weakness should result. Tibial shortening can be done, but there may be a residual bulkiness to the leg, and risks of nonunion and compartment syndrome are higher. If a tibial shortening is done, shortening over an IM nail and prophylactic compartment release are recommended. We limit the use of shortenings to 4 to 5 cm leg length inequality in patients who are skeletally mature.
Causes
The causes of LLD are many, including a previous injury, bone infection, bone diseases (dysplasias), inflammation (arthritis) and neurologic conditions. Previously broken bones may cause LLD by healing in a shortened position, especially if the bone was broken in many pieces (comminuted) or if skin and muscle tissue around the bone were severely injured and exposed (open fracture). Broken bones in children sometimes grow faster for several years after healing, causing the injured bone to become longer. Also, a break in a child?s bone through a growth center (located near the ends of the bone) may cause slower growth, resulting in a shorter extremity. Bone infections that occur in children while they are growing may cause a significant LLD, especially during infancy. Bone diseases may cause LLD, as well; examples are neurofibromatosis, multiple hereditary exostoses and Ollier disease. Inflammation of joints during growth may cause unequal extremity length. One example is juvenile rheumatoid arthritis. Osteoarthritis, the joint degeneration that occurs in adults, very rarely causes a significant LLD.
Symptoms
The most common symptom of all forms of LLD is chronic backache. In structural LLD the sufferer may also experience arthritis within the knee and hip are, flank pain, plantar fasciitis and metatarsalgia all on the side that is longer. Functional LLD sufferers will see similar conditions on the shorter side.
Diagnosis
Leg length discrepancy may be diagnosed during infancy or later in childhood, depending on the cause. Conditions such as hemihypertrophy or hemiatrophy are often diagnosed following standard newborn or infant examinations by a pediatrician, or anatomical asymmetries may be noticed by a child's parents. For young children with hemihypertophy as the cause of their LLD, it is important that they receive an abdominal ultrasound of the kidneys to insure that Wilm's tumor, which can lead to hypertrophy in the leg on the same side, is not present. In older children, LLD is frequently first suspected due to the emergence of a progressive limp, warranting a referral to a pediatric orthopaedic surgeon. The standard workup for LLD is a thorough physical examination, including a series of measurements of the different portions of the lower extremities with the child in various positions, such as sitting and standing. The orthopaedic surgeon will observe the child while walking and performing other simple movements or tasks, such as stepping onto a block. In addition, a number of x-rays of the legs will be taken, so as to make a definitive diagnosis and to assist with identification of the possible etiology (cause) of LLD. Orthopaedic surgeons will compare x-rays of the two legs to the child's age, so as to assess his/her skeletal age and to obtain a baseline for the possibility of excessive growth rate as a cause. A growth chart, which compares leg length to skeletal age, is a simple but essential tool used over time to track the progress of the condition, both before and after treatment. Occasionally, a CT scan or MRI is required to further investigate suspected causes or to get more sophisticated radiological pictures of bone or soft tissue.
Non Surgical Treatment
The object of treatment for leg length discrepancy is to level the pelvis and equalize the length of the two limbs. Inequalities of 2-2.5 centimeters can be handled with the following. Heel lifts/ adjustable heel lifts can be used inside a shoe where shoes have a full heel counter. Heel lifts may be added to the heel on the outside of the shoe along with an internal heel lift. Full platforms along the forefoot and rearfoot area of a shoe can be added. There are many different adjustable heel lifts available on the market. For treatment of a leg length discrepancy, consult your physician. They may refer you to a Physiotherapist or Chiropractor for determination of the type of LLD. A Certified Pedorthist (Canada) will treat a structural leg length discrepancy with a heel lift or in larger discrepancies a footwear modification.
how can a woman look taller?
Surgical Treatment
Surgeries for LLD are designed to do one of three general things ? shorten the long leg, stop or slow the growth of the longer or more rapidly growing leg, or lengthen the short leg. Stopping the growth of the longer leg is the most commonly utilized of the three approaches and involves an operation known as an epiphysiodesis , in which the growth plate of either the lower femur or upper tibia is visualized in the operating room using fluoroscopy (a type of real-time radiographic imaging) and ablated , which involves drilling into the region several times, such that the tissue is no longer capable of bone growth. Because the epiphyseal growth capabilities cannot be restored following the surgery, proper timing is crucial. Usually the operation is planned for the last 2 to 3 years of growth and has excellent results, with children leaving the hospital within a few days with good mobility. However, it is only appropriate for LLD of under 5cm.
Mortons Neuroma Cures
Overview
 Morton's neuroma (also known as Morton neuroma, Morton's metatarsalgia, Morton's neuralgia, plantar neuroma, intermetatarsal neuroma, and interdigital neuroma) is a benign neuroma of an intermetatarsal plantar nerve, most commonly of the second and third intermetatarsal spaces (between 2nd-3rd and 3rd-4th metatarsal heads), which results in the entrapment of the affected nerve. The main symptoms are pain and/or numbness, sometimes relieved by removing footwear.
Morton's neuroma (also known as Morton neuroma, Morton's metatarsalgia, Morton's neuralgia, plantar neuroma, intermetatarsal neuroma, and interdigital neuroma) is a benign neuroma of an intermetatarsal plantar nerve, most commonly of the second and third intermetatarsal spaces (between 2nd-3rd and 3rd-4th metatarsal heads), which results in the entrapment of the affected nerve. The main symptoms are pain and/or numbness, sometimes relieved by removing footwear.
Causes
There are a number of common causes for Morton?s Neuroma, (though the condition can arise spontaneously for reasons still unknown). The Neuroma often occurs in response to irritation, pressure or traumatic injury to one of the digital nerves leading to the toes. A thickening of nerve tissue results as part of the body?s response to the irritation or injury. Abnormal foot movement used to compensate for bunions, hammertoes, flatfeet and other conditions can lead to irritation and development of Morton?s Neuroma. Pronation of the foot may cause the heads of the metatarsal bones to rotate slightly, thereby pinching the nerve running between the metatarsal heads. Chronic pressure or pinching causes the nerve sheath to enlarge, becoming increasingly squeezed, producing worsening pain over time, if not addressed. Morton?s Neuroma can be exacerbated when tight shoes providing little room for the forefoot are worn. Activities which over-pronate the foot (such as walking barefoot in sand) may increase the pain associated with Morton?s Neuroma, as will any high-impact activity, such as jogging.
Symptoms
Morton's neuroma may cause Burning, pain, tingling, and numbness often shooting into the toes. Discomfort that is worse while walking. Feeling of a lump between the toes. Symptoms are usually temporarily relieved when taking off shoes, flexing toes or rubbing feet.
Diagnosis
Patients with classic Morton?s neuroma symptoms will have pain with pressure at the base of the involved toes (either between the 2nd and 3rd toes, or between the 3rd and 4th toes). In addition, squeezing the front of the foot together can exacerbate symptoms. As well, they may have numbness on the sides of one toe and the adjacent toe, as this corresponds with the distribution of the involved nerve.
Non Surgical Treatment
If symptoms are severe or persistent and self-help measures did not help, the doctor may recommend corticosteroid injections, a steroid medication that reduces inflammation and pain is injected into the area of the neuroma. Only a limited number of injections are advised, otherwise the risk of undesirable side effects increases, including hypertension (high blood pressure) and weight gain. Alcohol sclerosing injections, studies have shown that alcohol injections reduce the size of Morton's neuromas as well as alleviating pain. This is a fairly new therapy and may not be available everywhere. The doctor injects alcohol in the area of the neuroma to help sclerose (harden) the nerve and relieve pain. Injections are typically administered every 7 to 10 days. For maximum relief 4 to 7 injections are usually needed.
Surgical Treatment
Surgery for mortons neuroma consists of either a decompression, where more space is created for the nerve or a resection, where this part of the nerve is removed completely. This will result in some permanent minor numbness. Success rates for surgical procedures to treat mortons neuroma have a high success rate.
Morton's neuroma (also known as Morton neuroma, Morton's metatarsalgia, Morton's neuralgia, plantar neuroma, intermetatarsal neuroma, and interdigital neuroma) is a benign neuroma of an intermetatarsal plantar nerve, most commonly of the second and third intermetatarsal spaces (between 2nd-3rd and 3rd-4th metatarsal heads), which results in the entrapment of the affected nerve. The main symptoms are pain and/or numbness, sometimes relieved by removing footwear.Causes
There are a number of common causes for Morton?s Neuroma, (though the condition can arise spontaneously for reasons still unknown). The Neuroma often occurs in response to irritation, pressure or traumatic injury to one of the digital nerves leading to the toes. A thickening of nerve tissue results as part of the body?s response to the irritation or injury. Abnormal foot movement used to compensate for bunions, hammertoes, flatfeet and other conditions can lead to irritation and development of Morton?s Neuroma. Pronation of the foot may cause the heads of the metatarsal bones to rotate slightly, thereby pinching the nerve running between the metatarsal heads. Chronic pressure or pinching causes the nerve sheath to enlarge, becoming increasingly squeezed, producing worsening pain over time, if not addressed. Morton?s Neuroma can be exacerbated when tight shoes providing little room for the forefoot are worn. Activities which over-pronate the foot (such as walking barefoot in sand) may increase the pain associated with Morton?s Neuroma, as will any high-impact activity, such as jogging.
Symptoms
Morton's neuroma may cause Burning, pain, tingling, and numbness often shooting into the toes. Discomfort that is worse while walking. Feeling of a lump between the toes. Symptoms are usually temporarily relieved when taking off shoes, flexing toes or rubbing feet.
Diagnosis
Patients with classic Morton?s neuroma symptoms will have pain with pressure at the base of the involved toes (either between the 2nd and 3rd toes, or between the 3rd and 4th toes). In addition, squeezing the front of the foot together can exacerbate symptoms. As well, they may have numbness on the sides of one toe and the adjacent toe, as this corresponds with the distribution of the involved nerve.
Non Surgical Treatment
If symptoms are severe or persistent and self-help measures did not help, the doctor may recommend corticosteroid injections, a steroid medication that reduces inflammation and pain is injected into the area of the neuroma. Only a limited number of injections are advised, otherwise the risk of undesirable side effects increases, including hypertension (high blood pressure) and weight gain. Alcohol sclerosing injections, studies have shown that alcohol injections reduce the size of Morton's neuromas as well as alleviating pain. This is a fairly new therapy and may not be available everywhere. The doctor injects alcohol in the area of the neuroma to help sclerose (harden) the nerve and relieve pain. Injections are typically administered every 7 to 10 days. For maximum relief 4 to 7 injections are usually needed.
Surgical Treatment
Surgery for mortons neuroma consists of either a decompression, where more space is created for the nerve or a resection, where this part of the nerve is removed completely. This will result in some permanent minor numbness. Success rates for surgical procedures to treat mortons neuroma have a high success rate.
Shoe Lifts The Podiatrists Solution For Leg Length Imbalances
There are not one but two different types of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is structurally shorter in comparison to the other. As a result of developmental stages of aging, the brain picks up on the stride pattern and identifies some difference. Your body typically adapts by dipping one shoulder to the "short" side. A difference of under a quarter inch is not really excessive, require Shoe Lifts to compensate and typically doesn't have a serious effect over a lifetime.

Leg length inequality goes typically undiagnosed on a daily basis, yet this issue is easily remedied, and can eliminate numerous incidents of low back pain.
Therapy for leg length inequality typically consists of Shoe Lifts. They are low-priced, ordinarily priced at less than twenty dollars, compared to a custom orthotic of $200 or maybe more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Mid back pain is easily the most prevalent health problem afflicting people today. Over 80 million men and women have problems with back pain at some stage in their life. It's a problem which costs employers millions of dollars each year as a result of lost time and production. Fresh and improved treatment solutions are constantly sought after in the hope of lowering economic impact this condition causes.

Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In a lot of these cases Shoe Lifts are usually of very helpful. The lifts are capable of eliminating any pain and discomfort in the feet. Shoe Lifts are recommended by numerous skilled orthopaedic practitioners".
So that they can support the human body in a well-balanced fashion, feet have got a vital job to play. Despite that, it is often the most neglected region of the body. Many people have flat-feet which means there may be unequal force placed on the feet. This causes other areas of the body such as knees, ankles and backs to be affected too. Shoe Lifts ensure that correct posture and balance are restored.
Leg length inequality goes typically undiagnosed on a daily basis, yet this issue is easily remedied, and can eliminate numerous incidents of low back pain.
Therapy for leg length inequality typically consists of Shoe Lifts. They are low-priced, ordinarily priced at less than twenty dollars, compared to a custom orthotic of $200 or maybe more. When the amount of leg length inequality begins to exceed half an inch, a whole sole lift is generally the better choice than a heel lift. This prevents the foot from being unnecessarily stressed in an abnormal position.
Mid back pain is easily the most prevalent health problem afflicting people today. Over 80 million men and women have problems with back pain at some stage in their life. It's a problem which costs employers millions of dollars each year as a result of lost time and production. Fresh and improved treatment solutions are constantly sought after in the hope of lowering economic impact this condition causes.
Men and women from all corners of the world suffer from foot ache as a result of leg length discrepancy. In a lot of these cases Shoe Lifts are usually of very helpful. The lifts are capable of eliminating any pain and discomfort in the feet. Shoe Lifts are recommended by numerous skilled orthopaedic practitioners".
So that they can support the human body in a well-balanced fashion, feet have got a vital job to play. Despite that, it is often the most neglected region of the body. Many people have flat-feet which means there may be unequal force placed on the feet. This causes other areas of the body such as knees, ankles and backs to be affected too. Shoe Lifts ensure that correct posture and balance are restored.
The Diagnosis Of Calcaneal Spur

Overview
A heel spur is a projection or growth of bone where certain muscles and soft tissue structures of the foot attach to the bottom of the heel. Most commonly, the plantar fascia, a broad, ligament-like structure extending from the heel bone to the base of the toes becomes inflamed, and symptoms of heel pain begin. As this inflammation continues over a period of time, with or without treatment, a heel spur is likely to form. If heel pain is treated early, conservative therapy is often successful, and surgery is usually avoided.
Causes
A bone spur forms as the body tries to repair itself by building extra bone. It generally forms in response to pressure, rubbing, or stress that continues over a long period of time. Some bone spurs form as part of the aging process. As we age, the slippery tissue called cartilage that covers the ends of the bones within joints breaks down and eventually wears away (osteoarthritis). Bone spurs due to aging are especially common in the joints of the spine and feet.
Symptoms
The Heel Spur itself is not thought to be painful. Patients who experience pain with Plantar Fasciitis are suffering from inflammation and irritation of the plantar fascia. This the primary cause of pain and not the Heel Spur. Heel Spurs form in some patients who have plantar fasciitis, and tend to occur in patients who have had the problem for a prolonged period of time. While about 70 % of patients with plantar fasciitis have a heel spur, X-rays also show about 50 % of patients with no symptoms of plantar fasciitis also have a heel spur.
Diagnosis
Heel spurs and plantar fasciitis is usually diagnosed by your physiotherapist or sports doctor based on your symptoms, history and clinical examination. After confirming your heel spur or plantar fasciitis they will investigate WHY you are likely to be predisposed to heel spurs and develop a treatment plan to decrease your chance of future bouts. X-rays will show calcification or bone within the plantar fascia or at its insertion into the calcaneus. This is known as a calcaneal or heel spur. Ultrasound scans and MRI are used to identify any plantar fasciitis tears, inflammation or calcification. Pathology tests may identify spondyloarthritis, which can cause symptoms similar to plantar fasciitis.
Non Surgical Treatment
There are many temporary solutions to resolve the pain associated with irritation to the plantar ligaments. Common recommendations are ice and anti-inflammatory medications or even cortisone injections, however none of these solve the fundamental problem. To permanently resolve heel spurs you need to support and restrict the movement of the plantar ligaments. Flexible shoes will aggravate and often contribute to heel spurs. We recommend a RIGID orthotic that extends from the metatarsal heads to the heel to resolve heel spurs.
Surgical Treatment
In some cases, heel spurs are removed by surgery after an X-ray. While the surgery is typically effective, it?s a timely and expensive procedure. Even after surgery, heel spurs can re-form if the patient continues the lifestyle that led to the problem. These reasons are why most people who develop painful heel spurs begin looking for natural remedies for joint and bone pain. Surgery isn?t required to cure a heel spur. In fact, more than 90 percent of people get better with nonsurgical treatments. If nonsurgical methods fail to treat symptoms of heel spurs after 12 months, surgery may be necessary to alleviate pain and restore mobility.